This CPD Information email covers the Audit component of CPD.
Audit
Audit is a systematic critical analysis of the quality of surgical care that is reviewed by peers against explicit criteria or recognised standards.
The different types of audits one can undertake are
- Clinical Unit Audit
- Total Practice Audit
- Group of Speciality Audit
- Selected audit from surgical practice
- Clinical Registry
- Audit of reports (for surgeons who do not currently undertake surgery)
- Surgical Assistant Audit
Some background information about the Australian and New Zealand Audit of Surgical Mortality (ANZASM) – it is an independent external peer review of surgical mortality in various states and territories of Australia. The purpose of an audit is to review all deaths that occur during an episode of surgical care and to provide opportunities for improvements in patient outcomes.
https://www.surgeons.org/research-audit/surgical-mortality-audits
Overview
Each audit of surgical mortality is funded by its state or territory department of health (Western Australia, Victoria, South Australia, Queensland, Tasmania, Australian Capital Territory and Northern Territory) and is managed by RACS. For those states listed the ANZASM Steering Committee oversees the project which constitutes an invaluable foundation to the running and success of the audit program.
It is a RACS Continuing Professional Development (CPD) requirement to participate in the ANZASM if a surgeon is in operative based practice and experiences a surgical death, and an audit of surgical mortality is available in the surgeon's hospital.
Participation as a first or second line assessor remains voluntary and is encouraged.
The ANZASM publishes national case note review booklets and a case of the month: reading this contributes to CPD activities.
https://www.surgeons.org/research-audit/surgical-mortality-audits/national-case-note-reviews
For those of you in NSW, the Collaborating Hospitals Audit of Surgical Mortality (CHASM) provides comparable data to ANZASM, independently managed by the Clinical Excellence Commission of New South Wales.
For more information on CHASM - https://www.cec.health.nsw.gov.au/Review-incidents/mortality-review-authorised-committees/chasm
Participation in CHASM
- Surgeons can participate in CHASM by:
- completing a self-notification electronically through Fellows Interface Link (opening in Chrome recommended)
- submitting completed case forms for review
- completing peer review as a first-line assessor
- undertaking a detailed case note review as a second-line assessor
- becoming a member of the CHASM committee.
Hospitals can participate in CHASM by:
- submitting surgical deaths that meet the criteria stated in the Terms of Reference.
- The CHASM Office will create a case profile and generate a request to the operating surgeon to complete a case form.
- For hospitals, participation by surgeons in the program will ensure that deaths associated with surgical care undertake an independent peer review by a surgeon from the same specialty, with confidential feedback provided to the operating surgeon for their reflection.
Note for all, if you have had no surgical deaths, you need to acknowledge this on your RACS Portal.
Clinical Unit Audit
For surgeons who work in a public hospital with trainees / unaccredited registrars / medical officers:
There is generally a requirement for your clinical unit to undertake an audit of activities of the unit.
Some units may do a monthly audit, a 6 monthly audit, an annual audit of activities including surgical morbidity and mortality. This would include your surgery cases and participating in it by your cases and attending these audit meetings would fulfil the audit component.
You can enter the dates it covers as per the screenshots below

Select the competencies you want to apply for this audit:
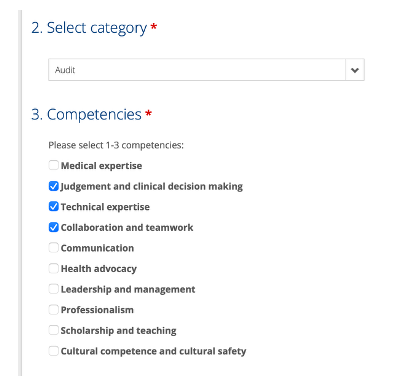
You can select different competencies for each audit:

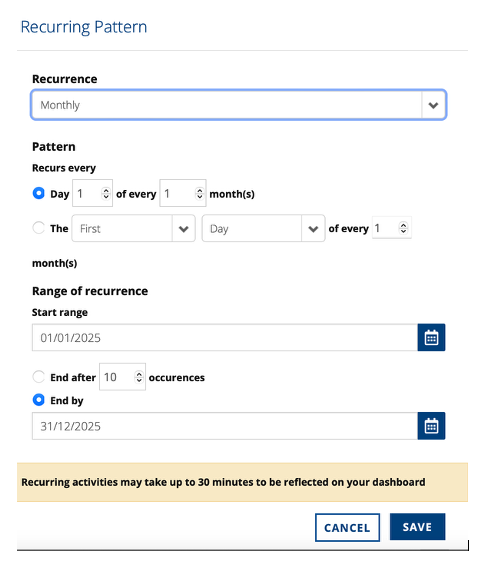
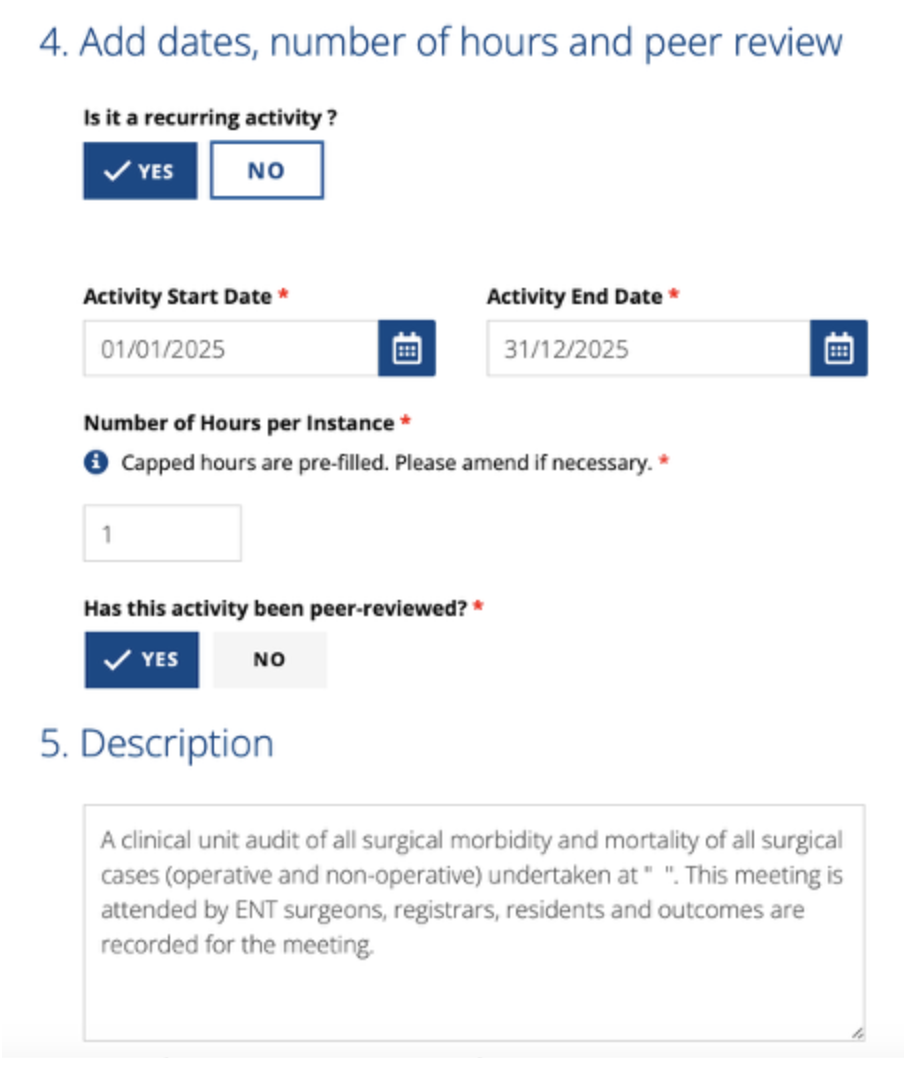
It can also be set up for the year ahead by adding dates, if it is recurring, and hours of audit undertaken. Select yes for the peer-review box.
Finally add a description of the audit activity. An example is provided below
You can upload minutes of the audit which will be generally acceptable if the attendees are recorded, the types of cases discussed, and agreed outcomes are documented.
For the surgeons solely in private practice, there are various types of audits that could be undertaken
It may be something straightforward for a selected audit e.g. number of tonsillectomies done, techniques, paediatric and adults, indications for surgery and post-tonsillectomy bleeding or readmissions for pain during the year. For those who are sub-specialised, it could be number of myringoplasty’s undertaken or number of revision FESS undertaken of your own primary cases.
If you are in a group practice, the surgeons in that group could undertake an audit of cases done by the group practice for a certain period or for the year, or selected types of procedures, and review these as part of your group’s regular business meetings.
If you are in solo practice, a suggestion is to undertake a similar audit of cases and present these results to a peer surgeon(s) for review.
Examples of tools to help you undertake an audit
https://www.surgeons.org/research-audit/morbidity-audits/morbidity-audit-services
Using Morbidity Audit and Logbook Tool (MALT)
Using a spreadsheet to enter cases. Recommended to code standardised outcomes (e.g 1= Yes, 2 = No, or 1 = Primary post tonsillectomy haemorrhage, 2 = secondary post tonsillectomy haemorrhage) to make it easier to analyse and collate outcomes against standard patient demographics (age, gender, tonsillectomy technique, date of surgery) rather than entering free text.
Once you have your 10 hours of audit there will be a green tick in your CPD dashboard:
Your 10 hours of audit can include the time you spend collecting and auditing your data and presenting your audit to a group of your peers. If the data from your cases is collected by your registrar on your behalf then record the hours for your audit as your attendance with discussion at the audit meeting with your peers.

Surgeons in non-operative or non-clinical roles
Surgeons who are working in non-operative or non-clinical roles are still required to complete a peer reviewed audit that related to their Area of Practice.
In the clinical setting, this may include an audit of non-operative consultations or medico-legal/clinical reports. In a non-clinical setting, this could include a review of student evaluations (teaching).
Fellows who are unsure how to meet this requirement can contact members@asohns.org.au or are encouraged to contact the RACS CPD Team to discuss their individual circumstances.
Contact RACS CPD on:
+61 3 9249 1282
cpd.college@surgeons.org